
Categories: Melanotan Peptides
 Sequence: Ac-Nle-Asp(1)-His-D-Phe-Arg-Trp-LyS(1)
Molecular Formula: CsHeN4O10
Molecular Weight: 1025.182 g/mol
PubChem ClD: 9941379
CAS Number: 189691-06-3
PT-141 Research
PT-141 and Sexual Arousa
PT-141 is a unique peptide in that it stimulates the MC-4R, which is known to producesexual arousal in the central nervous system and influence sexual behavior1, [2]. Studiesin mice have shown that agonist binding to MC-4R causes sexual arousal and increasedcopulation in both males and females[3], [4. Because PT-141 works via a differentmechanism than drugs like Viagra, it is possible to treat sexual arousal disorders in bothmen and women that stem from causes other than reduced blood flow to the genitals
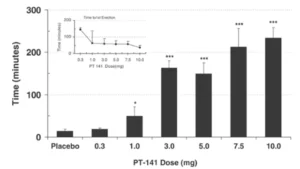
A study of men with erectile dysfunction (ED) who did not respond to sildenafil (Viagrafound that roughly one third experienced adequate erection for sexual intercourse withPT-141 (administered via nasal spray). There was also a strong dose-dependentresponse in the trial, indicating that PT-141 is indeed effective in certain casesl. Thissuggests that PT-141 could offer insight into correcting ED in settings where sildenafil hasfailed and may offer insight into central causes of hypoactive sexual desire.
Sequence: Ac-Nle-Asp(1)-His-D-Phe-Arg-Trp-LyS(1)
Molecular Formula: CsHeN4O10
Molecular Weight: 1025.182 g/mol
PubChem ClD: 9941379
CAS Number: 189691-06-3
PT-141 Research
PT-141 and Sexual Arousa
PT-141 is a unique peptide in that it stimulates the MC-4R, which is known to producesexual arousal in the central nervous system and influence sexual behavior1, [2]. Studiesin mice have shown that agonist binding to MC-4R causes sexual arousal and increasedcopulation in both males and females[3], [4. Because PT-141 works via a differentmechanism than drugs like Viagra, it is possible to treat sexual arousal disorders in bothmen and women that stem from causes other than reduced blood flow to the genitals
A study of men with erectile dysfunction (ED) who did not respond to sildenafil (Viagrafound that roughly one third experienced adequate erection for sexual intercourse withPT-141 (administered via nasal spray). There was also a strong dose-dependentresponse in the trial, indicating that PT-141 is indeed effective in certain casesl. Thissuggests that PT-141 could offer insight into correcting ED in settings where sildenafil hasfailed and may offer insight into central causes of hypoactive sexual desire.
 Interestingly, PT-141 was pulled from clinical trials before it reached approval for use inwomen suffering from HSDD. This is despite signs that the drug increased the number ofsatisfying sexual events per month and decreased female sexual distress scores in astatistically significant manner without any substantial side effectsls. Many experts whotreat female sexual dysfunction (FSD) were dismayed to find the peptide was not beingadvanced despite positive results. They point to a lack of established endpoints for trialsof FSD and socio-cultural biases against women’s sexual health as the primaryroadblocks that are inhibiting approval of what they see as much-needed therapies[4].They hope that greater attention will be given to the topic and that the FDA will establishmore concrete guidelines for evaluating therapies like PT-141 that can offer benefit.These experts also expressed dismay that the pharmacological treatments were nottested in conjunction with other established means of treating sexual dysfunction as theybelieve that the combination may prove synergistic and that peptides like PT-141 may beuseful for overcoming initial barriers and jump-starting psychological treatment modalities.
In 2017, partly in response to the outcry against the cessation of earlier trials, Phase llReconnect trials were launched using subcutaneous injections of PT-141 for FSD. Thenewest version of PT-141, called Rekynda, may soon be available for use in the UnitedStates. lt would be legal to use PT-141 off-label, at that point, to treat both male andfemale sexual dysfunction[8]. These new trials have relied on the kind of modifiedendpoints that experts in FSD have touted as beneficial to seeing these kinds oftreatments approved.
PT-141 and Hemorrhage
In 2009, PT-141 was modified slightly and investigated as a potential treatment forhemorrhagic shock. Because PT-141 binds to both MC-1R and MC-4R, it reducesischemia and protects tissues against inadequate blood supply in the setting ofhypovolemic (hemorrhagic) shock. The drug, when administered intravenously, does notproduce substantial side effects. lt was last in phase llb trials. The modified version of PT.141 is referred to as PL-6983.
PT-141 and infection
The MC-1R has been found, in a rat model of a specific fungal infection, to possessimportant anti-fungal and anti-inflammatory properties[9]. This is of particular importancebecause current anti-fungals are limited in terms of their mechanism of action and allproduce serious and treatment-limiting side effects in certain patients. Having analternative to use in the treatment of fungal infections could reduce morbidity andmortality substantially, especially in patients with immune compromise.
PT-141 and Cancer
The MC-1R receptor is an important stimulus of DNA repair pathways and thus is ofinterest in cancer treatment and preventionl[1o]. Research shows that people with variantsof MC-1R are at increased risk for both basal cell and sauamous cell carcinomaf1].Altered PT-141 may be able to correct the problems experienced as a result of thesevariants and prevent or treat these cancers.
Research Directions
Right now, PT-141 hIs received widespread and intense attention as a treatment forsexual dysfunction.here is, however, a great deal of potential research outside of sexualdysfunction and hemorrhage that PT-141 could be applied to. For instance, MC-4R isective or missing in certain cases of obesity and may account for aswell-known to be defmuch as 6% of all cases of early-onset obesity. PT-141 offers a unique means ofexploring this particuar cause of obesity and potentially illustrating a pathway forintervention.MC-1Rblays roles in both pain and inflammation as well as kidneyead of infection. There is a plethora of available research that PT.pathology and the sp141 could help to shd light on.
PT-141 exhibits minimal side effects, low oral and excellent subcutaneous bioavailabilityin mice. Per kg dosage in mice does not scale to humans. PT-141 for sale at PeptideSciences is limited to educational and scientific research only, not for humanconsumption. Only buy PT-141 if you are a licensed researcher.
Article Author
The above literature was researched, edited and organized by Dr. Logan, M.D. Dr. Loganholds a doctorate degree from Case Western Reserve University School of Medicine anda B.S. in molecular biology.
Scientific Journal Author
Dr. Sheryl A. Kingsberg is the chief of behavioral medicine at University Hospitals CaseMedical Center and professor in Reproductive Biology and Psychiatry at Case WesternReserve University. Her areas of clinical specialization include sexual medicine, femalesexual disorders, cognitive behavioral psychotherapy, menopause, pregnancy andpostpartum mood disorders, psychological aspects of infertility, and psychological andsexual aspects of cancer. Dr. Kingsberg’s primary research interests are in treatments forfemale sexual disorders and the psychological aspects of infertility and menopause. Sheled a randomized, placebo-controlled dose-findina trial for PT-141, She has numerouspublications in many national and internationa iournals, sits on the editoria board ofMenopause and has authored numerous chapters on topics incudina perimenopauseand sexuality, oocyte donation, infertility and aging, the treatment of psychogenic erectiledysfunction and sexuality after cancer. Dr. Kingsberg received her PhD from theUniversity of South Florida in Tampa and completed her fellowship in sexual medicine atUniversity Hospitals Case Medical Center. She is an active member in a number ofnational and international organizations including the American Psychological Associationand the American Society for Reproductive Medicine, She currently sits on the Board ofTrustees of The North American Menopause Society, and serves as the current treasurerof the Society for Assisted Reproductive Technologies, Dr, Kingsberg s a past president oThe International Society for the Study of Women’s Sexual Health.
Dr. Sheryl A. Kingsberg is being referenced as one of the leading scientists involved inthe research and development of PT-141. in no way is this doctor/scientist endorsing oradvocating the purchase, sale, or use of this product for any reason. There is no affiliationor relationship, implied or otherwise, between PEPTIDE GURUS and this doctor. Thepurpose of citing the doctor is to acknowledge, recognize, and credit the exhaustiveresearch and development efforts conducted by the scientists studying this peptide. Dr.Kingsberg is listed in [12] under the referenced citations.
Referenced Citations
1.M.Sandrock, A.Schulz,C.Merkwitz,T.Schöneberg, K.Spanel-Borowski, and ARicken,“Reduction in corpora lutea number in obese melanocortin-4-receptor-deficient mice,”Reprod. Biol. Endocrinol. RBE, vol.7, p. 24, Mar. 2009.
2.R.C.Rosen,L.E.Diamond,D.C.Earle,A. M. Shadiack, and P. B. Molinoff’Evaluation of the safety, pharmacokinetics and pharmacodynamic effects ofsubcutaneously administered PT-141, a melanocortin receptor agonist, in healthymale subiects and in patients with an inadeauate response to Viagra,” Int. J. lmpotRes.,vol.16,no.2,pp.135-142,Apr. 2004.[PubMed]
3.H.Wessells, V. J. Hruby, J. Hackett, G. Han, P. Balse-Srinivasan, and T. W.Vanderah, “Ac-Nle-cAsp-His-DPhe-Arg-Trp-Lys]-NH2 induces penile erection viabrain and spinal melanocortin receptors,” Neuroscience, vol. 118, no. 3, pp. 755-762,2003.[PubMed]
4.A.-S.Rössler, J.G. Pfaus, H. K. Kia, J. Bernabé, L.Alexandre, and F. Giuliano,“The melanocortin agonist, melanotan ll, enhances proceptive sexual behaviors inthe female rat,”Pharmacol. Biochem. Behav., vol. 85, no.3, pp.514-521, NOv.2006.[PubMed]
5.M.R. Safarinejad and S.Y. Hosseini, “Salvage of sildenafil failures withbremelanotide: a randomized, double-blind, placebo controlled study,” J. Urol., vol179,no.3, pp.1066-1071,Mar. 2008.[PubMed]
6.A. H. Clayton et al., “Bremelanotide for female sexual dysfunctions inpremenopausal women: a randomized, placebo-controlled dose-finding trial,Womens Health Lond.Engl., vol.12, no.3, pp.325-337,2016.[PubMed]
7.M.K. Miller, J.R. Smith, J.J. Norman, and A. H. Clayton,“Expert opinion onexisting and developing drugs to treat female sexual dysfunction,” Expert Opin.Emerg.Drugs,vol.23,no.3,pp.223-230,2018.[PubMed]
8.“AMAG Pharmaceuticals and Palatin Technologies Enter Into Exclusive LicensingAgreement for North American Rights to RekyndaTM (bremelanotide), a PotentialTreatment for a Common Female Sexual Disorder -AMAG Pharmaceuticals.[MarketWatch]
9.H. Ji et al., “The Synthetic Melanocortin (CKPV)2 Exerts Anti-Fungal and Anti-Inflammatory Effects against Candida albicans Vaginitis via Inducing MacrophageM2 Polarization,”PLoS ONE, vol.8, no.2, Feb.2013.[PLOS ONE]
10.V. Maresca, E. Flori, and M. Picardo, “Skin phototype: a new perspective,” PigmentCell Melanoma Res., vol.28,no.4,pp.378-389, Jul.2015.[PubMed]
11.L. Feller, R. a. G. Khammissa, B. Kramer, M. Altini, and J. Lemmer, “Basal cellcarcinoma, squamous cell carcinoma and melanoma of the head and face,” HeadFace Med.. vol.12,p.11,Feb.2016.[PubMed]
12.Clayton AH, Althof SE, Kingsberg S, et al. Bremelanotide for female sexualdysfunctions in premenopausal women: a randomized, placebo-controlled dose-finding trial.Womens Health (Lond).2016;12(3):325-337.doi:10.2217/whe-2016-0018
13.T. R. McMilan, M. A. M. Forster, L. 1. Short, A. P. Rudecki, D. L. Cline, and S. L.Gray, “Melanotan ll, a melanocortin agonist, partially rescues the impairedthermogenic capacity of pituitary adenylate cyclase-activating polypeptide deficientmice,Exp.Physiol. ,vol.106,no.2,pp.427-437,Feb.2021, doi:10.1113/EP088838.”
14.C. Spana, R. Jordan, and S. Fischkoff, “Effect of bremelanotide on body weight ofobese women: Data from two phase 1 randomized controlled trials,Diabetes Obes.Metab., vol.24,no.6, pp.1084-1093, Jun.2022, doi: 10.1111/dom.14672·”
ALL ARTICLES AND PRODUCT INFORMATION PROVIDED ON THIS WEBSITE AREFOR INFORMATONAL AND EDUCATIONAL PURPOSES ONLY.
The products offered on this website are furnished for in-vitro studies only. in-vitro studies(Latin: in glass) are performed outside of the body. These products are not medicines ordrugs and have not been approved by the FDA to prevent, treat or cure any medicalcondition, ailment or disease, Bodily introduction of any kind into humans or animals isstrictly forbidden by law.
Interestingly, PT-141 was pulled from clinical trials before it reached approval for use inwomen suffering from HSDD. This is despite signs that the drug increased the number ofsatisfying sexual events per month and decreased female sexual distress scores in astatistically significant manner without any substantial side effectsls. Many experts whotreat female sexual dysfunction (FSD) were dismayed to find the peptide was not beingadvanced despite positive results. They point to a lack of established endpoints for trialsof FSD and socio-cultural biases against women’s sexual health as the primaryroadblocks that are inhibiting approval of what they see as much-needed therapies[4].They hope that greater attention will be given to the topic and that the FDA will establishmore concrete guidelines for evaluating therapies like PT-141 that can offer benefit.These experts also expressed dismay that the pharmacological treatments were nottested in conjunction with other established means of treating sexual dysfunction as theybelieve that the combination may prove synergistic and that peptides like PT-141 may beuseful for overcoming initial barriers and jump-starting psychological treatment modalities.
In 2017, partly in response to the outcry against the cessation of earlier trials, Phase llReconnect trials were launched using subcutaneous injections of PT-141 for FSD. Thenewest version of PT-141, called Rekynda, may soon be available for use in the UnitedStates. lt would be legal to use PT-141 off-label, at that point, to treat both male andfemale sexual dysfunction[8]. These new trials have relied on the kind of modifiedendpoints that experts in FSD have touted as beneficial to seeing these kinds oftreatments approved.
PT-141 and Hemorrhage
In 2009, PT-141 was modified slightly and investigated as a potential treatment forhemorrhagic shock. Because PT-141 binds to both MC-1R and MC-4R, it reducesischemia and protects tissues against inadequate blood supply in the setting ofhypovolemic (hemorrhagic) shock. The drug, when administered intravenously, does notproduce substantial side effects. lt was last in phase llb trials. The modified version of PT.141 is referred to as PL-6983.
PT-141 and infection
The MC-1R has been found, in a rat model of a specific fungal infection, to possessimportant anti-fungal and anti-inflammatory properties[9]. This is of particular importancebecause current anti-fungals are limited in terms of their mechanism of action and allproduce serious and treatment-limiting side effects in certain patients. Having analternative to use in the treatment of fungal infections could reduce morbidity andmortality substantially, especially in patients with immune compromise.
PT-141 and Cancer
The MC-1R receptor is an important stimulus of DNA repair pathways and thus is ofinterest in cancer treatment and preventionl[1o]. Research shows that people with variantsof MC-1R are at increased risk for both basal cell and sauamous cell carcinomaf1].Altered PT-141 may be able to correct the problems experienced as a result of thesevariants and prevent or treat these cancers.
Research Directions
Right now, PT-141 hIs received widespread and intense attention as a treatment forsexual dysfunction.here is, however, a great deal of potential research outside of sexualdysfunction and hemorrhage that PT-141 could be applied to. For instance, MC-4R isective or missing in certain cases of obesity and may account for aswell-known to be defmuch as 6% of all cases of early-onset obesity. PT-141 offers a unique means ofexploring this particuar cause of obesity and potentially illustrating a pathway forintervention.MC-1Rblays roles in both pain and inflammation as well as kidneyead of infection. There is a plethora of available research that PT.pathology and the sp141 could help to shd light on.
PT-141 exhibits minimal side effects, low oral and excellent subcutaneous bioavailabilityin mice. Per kg dosage in mice does not scale to humans. PT-141 for sale at PeptideSciences is limited to educational and scientific research only, not for humanconsumption. Only buy PT-141 if you are a licensed researcher.
Article Author
The above literature was researched, edited and organized by Dr. Logan, M.D. Dr. Loganholds a doctorate degree from Case Western Reserve University School of Medicine anda B.S. in molecular biology.
Scientific Journal Author
Dr. Sheryl A. Kingsberg is the chief of behavioral medicine at University Hospitals CaseMedical Center and professor in Reproductive Biology and Psychiatry at Case WesternReserve University. Her areas of clinical specialization include sexual medicine, femalesexual disorders, cognitive behavioral psychotherapy, menopause, pregnancy andpostpartum mood disorders, psychological aspects of infertility, and psychological andsexual aspects of cancer. Dr. Kingsberg’s primary research interests are in treatments forfemale sexual disorders and the psychological aspects of infertility and menopause. Sheled a randomized, placebo-controlled dose-findina trial for PT-141, She has numerouspublications in many national and internationa iournals, sits on the editoria board ofMenopause and has authored numerous chapters on topics incudina perimenopauseand sexuality, oocyte donation, infertility and aging, the treatment of psychogenic erectiledysfunction and sexuality after cancer. Dr. Kingsberg received her PhD from theUniversity of South Florida in Tampa and completed her fellowship in sexual medicine atUniversity Hospitals Case Medical Center. She is an active member in a number ofnational and international organizations including the American Psychological Associationand the American Society for Reproductive Medicine, She currently sits on the Board ofTrustees of The North American Menopause Society, and serves as the current treasurerof the Society for Assisted Reproductive Technologies, Dr, Kingsberg s a past president oThe International Society for the Study of Women’s Sexual Health.
Dr. Sheryl A. Kingsberg is being referenced as one of the leading scientists involved inthe research and development of PT-141. in no way is this doctor/scientist endorsing oradvocating the purchase, sale, or use of this product for any reason. There is no affiliationor relationship, implied or otherwise, between PEPTIDE GURUS and this doctor. Thepurpose of citing the doctor is to acknowledge, recognize, and credit the exhaustiveresearch and development efforts conducted by the scientists studying this peptide. Dr.Kingsberg is listed in [12] under the referenced citations.
Referenced Citations
1.M.Sandrock, A.Schulz,C.Merkwitz,T.Schöneberg, K.Spanel-Borowski, and ARicken,“Reduction in corpora lutea number in obese melanocortin-4-receptor-deficient mice,”Reprod. Biol. Endocrinol. RBE, vol.7, p. 24, Mar. 2009.
2.R.C.Rosen,L.E.Diamond,D.C.Earle,A. M. Shadiack, and P. B. Molinoff’Evaluation of the safety, pharmacokinetics and pharmacodynamic effects ofsubcutaneously administered PT-141, a melanocortin receptor agonist, in healthymale subiects and in patients with an inadeauate response to Viagra,” Int. J. lmpotRes.,vol.16,no.2,pp.135-142,Apr. 2004.[PubMed]
3.H.Wessells, V. J. Hruby, J. Hackett, G. Han, P. Balse-Srinivasan, and T. W.Vanderah, “Ac-Nle-cAsp-His-DPhe-Arg-Trp-Lys]-NH2 induces penile erection viabrain and spinal melanocortin receptors,” Neuroscience, vol. 118, no. 3, pp. 755-762,2003.[PubMed]
4.A.-S.Rössler, J.G. Pfaus, H. K. Kia, J. Bernabé, L.Alexandre, and F. Giuliano,“The melanocortin agonist, melanotan ll, enhances proceptive sexual behaviors inthe female rat,”Pharmacol. Biochem. Behav., vol. 85, no.3, pp.514-521, NOv.2006.[PubMed]
5.M.R. Safarinejad and S.Y. Hosseini, “Salvage of sildenafil failures withbremelanotide: a randomized, double-blind, placebo controlled study,” J. Urol., vol179,no.3, pp.1066-1071,Mar. 2008.[PubMed]
6.A. H. Clayton et al., “Bremelanotide for female sexual dysfunctions inpremenopausal women: a randomized, placebo-controlled dose-finding trial,Womens Health Lond.Engl., vol.12, no.3, pp.325-337,2016.[PubMed]
7.M.K. Miller, J.R. Smith, J.J. Norman, and A. H. Clayton,“Expert opinion onexisting and developing drugs to treat female sexual dysfunction,” Expert Opin.Emerg.Drugs,vol.23,no.3,pp.223-230,2018.[PubMed]
8.“AMAG Pharmaceuticals and Palatin Technologies Enter Into Exclusive LicensingAgreement for North American Rights to RekyndaTM (bremelanotide), a PotentialTreatment for a Common Female Sexual Disorder -AMAG Pharmaceuticals.[MarketWatch]
9.H. Ji et al., “The Synthetic Melanocortin (CKPV)2 Exerts Anti-Fungal and Anti-Inflammatory Effects against Candida albicans Vaginitis via Inducing MacrophageM2 Polarization,”PLoS ONE, vol.8, no.2, Feb.2013.[PLOS ONE]
10.V. Maresca, E. Flori, and M. Picardo, “Skin phototype: a new perspective,” PigmentCell Melanoma Res., vol.28,no.4,pp.378-389, Jul.2015.[PubMed]
11.L. Feller, R. a. G. Khammissa, B. Kramer, M. Altini, and J. Lemmer, “Basal cellcarcinoma, squamous cell carcinoma and melanoma of the head and face,” HeadFace Med.. vol.12,p.11,Feb.2016.[PubMed]
12.Clayton AH, Althof SE, Kingsberg S, et al. Bremelanotide for female sexualdysfunctions in premenopausal women: a randomized, placebo-controlled dose-finding trial.Womens Health (Lond).2016;12(3):325-337.doi:10.2217/whe-2016-0018
13.T. R. McMilan, M. A. M. Forster, L. 1. Short, A. P. Rudecki, D. L. Cline, and S. L.Gray, “Melanotan ll, a melanocortin agonist, partially rescues the impairedthermogenic capacity of pituitary adenylate cyclase-activating polypeptide deficientmice,Exp.Physiol. ,vol.106,no.2,pp.427-437,Feb.2021, doi:10.1113/EP088838.”
14.C. Spana, R. Jordan, and S. Fischkoff, “Effect of bremelanotide on body weight ofobese women: Data from two phase 1 randomized controlled trials,Diabetes Obes.Metab., vol.24,no.6, pp.1084-1093, Jun.2022, doi: 10.1111/dom.14672·”
ALL ARTICLES AND PRODUCT INFORMATION PROVIDED ON THIS WEBSITE AREFOR INFORMATONAL AND EDUCATIONAL PURPOSES ONLY.
The products offered on this website are furnished for in-vitro studies only. in-vitro studies(Latin: in glass) are performed outside of the body. These products are not medicines ordrugs and have not been approved by the FDA to prevent, treat or cure any medicalcondition, ailment or disease, Bodily introduction of any kind into humans or animals isstrictly forbidden by law. PeptideGurus is a leading supplier of American-made research peptides, offering top-quality products at competitive prices. With a focus on excellence and customer service, they ensure a secure and convenient ordering process with global shipping.
© Copyright Peptide Gurus 2024. All rights reserved.Privacy Policy
All products on this site are for Research, Development use only. Products are Not for Human consumption of any kind. The statements made within this website have not been evaluated by the US Food and Drug Administration or HEALTH CANADA. The statements and the products of this company are not intended to diagnose, treat, cure or prevent any disease.
PeptideGurus is a chemical supplier. PeptideGurus is not a compounding pharmacy or chemical compounding facility as defined under 503A of the Federal Food, Drug, and Cosmetic act. Peptide Sciences is not an outsourcing facility as defined under 503B of the Federal Food, Drug, and Cosmetic act.
CONTACT



